
 Idebenone (pronounced eye deb e known) is a synthetic analog (variant) of one of life's most essential biochemicals, coenzyme Q10 (Co Q10). Co Q10 is an important antioxidant component of the lipid (fatty) membranes that surround all cells, as well as the lipid membranes surrounding the various organelles ("little organs"), such as mitochondria and microsomes, inside cells.
Idebenone (pronounced eye deb e known) is a synthetic analog (variant) of one of life's most essential biochemicals, coenzyme Q10 (Co Q10). Co Q10 is an important antioxidant component of the lipid (fatty) membranes that surround all cells, as well as the lipid membranes surrounding the various organelles ("little organs"), such as mitochondria and microsomes, inside cells.
Co Q10 is also an important member of the "Electron Transport Chain" (ETC) within mitochondria, which are the "power plants" of the cell. Most of the oxygen we breathe is used inside the electron transport chain to produce much of the ATP bioenergy that powers virtually every activity of our cells and bodies.
Co Q10’s pro-oxidant action
 When blood flow is seriously reduced to any part of the body, as in a heart attack, stroke, trauma, shock, or chronic poor blood circulation- cellular/ mitochondrial oxygen (O2) levels quickly drop in the affected region. Yet because oxygen is seven to eight times more soluble in the lipid zones of cell membrane, compared to the watery compartments of the cell, there is still sufficient oxygen remaining in the membranes of cells and organelles, as well as in the electron transport chain, to auto-oxidize Co Q10. As the Co Q10 auto-oxidizes, hydrogen peroxide, superoxide and hydroxl free radicals are rapidly formed in massive numbers. These free radicals quickly damage cell/ organelle structure and function, as well as rapidly halt ATP energy generation by the electron transport chain.
When blood flow is seriously reduced to any part of the body, as in a heart attack, stroke, trauma, shock, or chronic poor blood circulation- cellular/ mitochondrial oxygen (O2) levels quickly drop in the affected region. Yet because oxygen is seven to eight times more soluble in the lipid zones of cell membrane, compared to the watery compartments of the cell, there is still sufficient oxygen remaining in the membranes of cells and organelles, as well as in the electron transport chain, to auto-oxidize Co Q10. As the Co Q10 auto-oxidizes, hydrogen peroxide, superoxide and hydroxl free radicals are rapidly formed in massive numbers. These free radicals quickly damage cell/ organelle structure and function, as well as rapidly halt ATP energy generation by the electron transport chain.
Brain and spinal cord cells are especially prone to such damage, and may be irreparably damaged or even destroyed within minutes.
Why Idebenone is superior to Co Q10
Enter Idebenone to the rescue! Studies have shown that under the same cellular low oxygen conditions that cause Co Q10 to act as a pro-oxidant producer of damaging free radicals, Idebenone prevents the free radical dam-age and maintains relatively normal cell ATP levels. In short, while Idebenone can effectively substitute for Co Q10's positive and life essential functions, it doesn't have Co Q10's free radical producing and energy crashing "dark side" which occurs under hypoxic (low oxygen) conditions.
Idebenone's potential benefits fall into five categories; antiaging, energy enhancement, cognition enhancement, organ protector and protector against excitatory amino acid neurotoxicity.
Idebenone – The anti-aging benefits
The mitochondrial power plants produce over 90% of all cellular ATP bioenergy. They are also generally the richest sites in Co Q10 (or Idebenone). Mitochondrial DNA (mtDNA) allows mitochondria to reproduce them-selves.
While the DNA in a cell nucleus comes from both our parents, mtDNA comes exclusively from our mother's mtDNA.
There are typically two or three copies of mtDNA in each mitochondrion, with average 1000 mitochondria per cell. Because mtDNA exists in the "heart of the fiery furnace" where electron "sparks" are constantly leaking as ATP is produced in the electron transport chain, mtDNA is far more prone to free radical electron damage than is the DNA in our cell nuclei that contains the "blueprint" for our entire organism.
At the same time, the repair capacity of mtDNA is much less than that of our cell nucleus DNA. As a consequence, over the course of a lifetime our mtDNA becomes ever more damaged, and the mitochondria produced therefrom become ever more ineffective at energy generation.
Studies comparing heart tissue from young people with that from elderly people have shown almost no significant mitochondrial dysfunction in young hearts, with significant, often severe mitochondrial dysfunction in elderly hearts.
The cells that are most susceptible to mitochondrial energy depletion with advancing age are the brain, skeletal muscle and heart muscle cells. Idebenone thus offers a prime anti-aging effect here in several ways. Unlike Co Q10, even under the low oxygen conditions that may occur periodically over a lifetime, Idebenone will serve as a powerful mitochondrial free radical quencher, lessening the ever-increasing mtDNA damage that occurs with age. Idebenone will work even better than Co Q10 within the electron transport chain to keep energy production high, even under hypoxic conditions. This is especially critical to brain and heart cells that may be rapidly damaged during low ATP production episodes that occur due to poor tissue oxygenation.
Idebenone – Energy enhancement
 Iron is a "dual edged sword." It is absolutely essential for life, it plays a central role in ATP generation in the electron transport chain. Yet iron can also be a powerful initiator of free radical production and cell structural damage, especially under low oxygen conditions.
Iron is a "dual edged sword." It is absolutely essential for life, it plays a central role in ATP generation in the electron transport chain. Yet iron can also be a powerful initiator of free radical production and cell structural damage, especially under low oxygen conditions.
This occurs, for example, during stroke, and during the gradual onset of Parkinson's disease. Studies have shown that Idebenone can tightly couple oxidation to energy production. This prevents iron ions from wastefully and toxically, diverting oxygen to producing free radicals inside the mitochondria, instead of energy.
Studies have shown that Idebenone can almost completely eliminate this, diverting 10% of cellular oxygen away from toxic iron induced free radical generation, to beneficial ATP energy production under hypoxic conditions.
Mild cellular hypoxia can occur even from intense exercise, or even from mild exercise done by out of shape "couch potatoes."
Idebenone – Cognition enhancement
A variety of studies using brain cells, (animal and humans) have shown Idebenone's ability to enhance brain structure and function.
Human and animal studies have demonstrated that Idebenone can enhance serotonin production, even under far less than optimal conditions, as e.g. with a very low tryptophan diet, or in patients with cerebrovascular dementia.
Idebenone has enhanced cholinergic nerve function and consequent learning ability even under hypoxic conditions, or when an anti-cholinergic drug (Scopolamine) was administered.
Idebenone has increased cellular catecholamine (dopamine, adrenalin and noradrenanlin) production by enhancing cellular uptake of the precursor amino-acid tyrosine.
Idebenone enhances long term potentiation in hippocampal nerve cells, a key part of memory formation and consolidation. Idebenone has restored glucose (brain fuel) utilization and ATP production in ischemic (poor blood flow) rat-brain.
Idebenone has been shown to enhance general cerebral metabolism, lessen the damage from strokes, and has been used to treat Alzheimer's and other dementias.
And like the original nootropic drug; piracetam, Idebenone has been shown to promote information transfer across the corpus callosum, the membrane separating the right and left brain hemispheres.
This is turn may promote the union/ integration of the logical (yang) and intuitive (yin) halves of the brain/ mind.
Idebenone – Organ protector
As our organs age or are damaged, we age and are damaged. Over a lifetime, blood flow to our organs diminishes due to arteriosclerosis and less efficient heart pumping. This reduces oxygen dependent energy production needed for repair, reproduction and normal function of the organ cells. Free radical damage accumulates over time, leaving ever more dead, dying or dysfunctional cells within organs.
At some point a critical threshold is reached when too many cells within an organ are dysfunctional, and they can no longer sustain the organ's life and function. Then the organ- heart, brain, liver etc. fails.
Idebenone protects organs in many ways, it cushions them against hypoxic (low oxygen) and/ or ischemic (poor blood flow) damage. Idebenone enhances both normal and hypoxic ATP energy generation.
Each cell in our organs must produce the energy it needs for life and health, cells cannot "borrow" energy from each other.
Idebenone – The free radical quencher
Idebenone is a powerful antioxidant, more so than Co Q10, and in some studies is 30 to 100 times more effective, than vitamin E or vinpocetine as a free radical quencher within the brain cells.
Idebenone lessens the free radical induced mtDNA damage that accumulates acceleratingly over a lifetime, slowing organ damage and aging.
A 1995 study in the Journal of Transplantation compared the organ preserving effects of Co Q10 and Idebenone. The study measured various factors, such as free radical membrane lipid damage, cell protein damage and cellular energy production under hypoxia conditions.
The results showed Idebenone to be dramatically more effective than Co Q10 at preserving liver tissue under conditions identical to that endured by whole livers "harvested" and stored (briefly) before transplant to another person.
The study recommended using Idebenone to increase the transplant viability of human livers donated for organ transplant. Why not use Idebenone to increase your own organ viability, while you still have the use of them!
Protection against excitatory amino acid (EAA) neuro toxicity
Glutamic acid and aspartic acid are the two chief excitatory amino acid neurotransmitters in the human brain. Without them we would be "mental vegetables."
Yet under certain conditions, e.g. stroke or traumatic brain injury- excessive amounts of excitatory amino acids accumulate in the fluid surrounding brain cells, causing damage and even death to nerve and glial cells through free radical mechanisms.
Excitatory amino acid toxicity is at least partly responsible for the neurotoxicity of the recreational drug "Ecstasy or MDMA." Studies over the past 30 years have also shown that excessive dietary intake of excitatory amino acids may also damage brain structure/ function, especially in children or excitatory amino acid sensitive adults.
The two main dietary sources of excitatory amino acids are the flavor enhancer MSG (monosodium glutamate) and the artificial sweetener aspartame (Nutrasweet). Also many processed foods (e.g. canned soups, dry roasted spiced peanuts, beef/ chicken bouillon, canned tuna, spices etc.) contain "hydrolized vegetable protein, yeast extract, soy protein isolate" and similar ingredients that are mostly excitatory amino acids.
In studies with various types of nerve cell, as well as oligodendroglial cells (which make up the protective myelin sheaths surrounding many nerves, the so-called "white matter" of the brain). Idebenone has shown dramatic protective effects against glutamate toxicity.
So who can benefit from Idebenone? The answers are,
1. Healthy people wishing cognitive enhancement and brain energizer effects (it synergizes well with piracetam, vinpocetine and Hydergine). 2 or 3 tablets (45mg each) daily.
2. Stroke victims wishing to improve memory, emotional or speech disturbances. 3 to 6 tablets (45mg each) daily.
3. Alzheimer's and cerebrovascular dementia patients. 4 to 6 tablets (45mg each) daily.
4. Those preparing for major surgery, especially brain, heart, liver or kidney. Synergizes well with Hydergine. 4 to 6 tablets (45mg each).
5. People with heart energetics problems, e.g. cardiomyopathy, ischemic heart disease, congestive heart failure. 3 to 6 tablets (45mg each) daily.
6. People with myelination problems, e.g. multiple sclerosis or "white matter" stroke injury. 3 to 6 tablets (45mg each) daily.
7. Those seeking to increase their general energy and vitality levels. 2 to 3 tablets (45mg each) daily.
8. People with especially high endurance energy needs, e.g. cross country skiers, long distance runners, cyclists, swimmers etc. 3 to 4 tablets (45mg each) daily.
9. Those at risk of excitatory amino acid brain damage, e.g. people who routinely consume large amounts of aspartame sweetened foods/ drinks, or those who routinely eat MSG or "hydrolyzed vegetable protein" containing restaurant or prepared foods. 2 or 3 tablets (45mg each) daily.
10. People wishing to enhance the brain serotonin benefits of tryptophan or 5-hydroxy-tryptophan supplements or SSRI drugs, such as Prozac, Paxil, Zoloft, or Luvox etc. 2 to 4 tablets (45mg each) daily.
11. Those suffering acute or chronic liver damage from poison mushrooms, toxic chemicals, hepatitis etc. 2 to 4 tablets (45mg each) daily.
Numerous studies have shown that idebenone is well distributed through-out the body after absorption, accumulating in cellular and organelle membranes, as well as in the electron transport chain, exactly where it does the most good!



 Washington, Oct 13 : It seems that the troubled movie star Owen Wilson has taken solace in ancient Native American remedies in order to get rid of the
Washington, Oct 13 : It seems that the troubled movie star Owen Wilson has taken solace in ancient Native American remedies in order to get rid of the 


 Tropic Thunder was scheduled to shoot in several weeks. Other in-the-works projects such as Drillbit Taylor and Marley & Me are progressing as scheduled. Meanwhile, Owen's friends and colleagues have been quiet, awaiting his lead.
Tropic Thunder was scheduled to shoot in several weeks. Other in-the-works projects such as Drillbit Taylor and Marley & Me are progressing as scheduled. Meanwhile, Owen's friends and colleagues have been quiet, awaiting his lead.



 Dorothy Hamill still has it: the sparkling charm, and the athletic grace that won her Olympic gold in 1976. Her dazzling smile made her America's sweetheart when she won figure skating gold in the 1976 Winter Olympics in Innsbruck, Austria. At nineteen years old, Hamill was thrust into the spotlight and mobbed for autographs. She was a star, but she didn't feel like one. "When you have that goal and you have that dream and it actually happens, you think that it would be a switch," she told CBS News correspondent Thalia Assuras. "And that all of a sudden you'd feel, you know, like an Olympic champion. And I didn't feel any different."
Dorothy Hamill still has it: the sparkling charm, and the athletic grace that won her Olympic gold in 1976. Her dazzling smile made her America's sweetheart when she won figure skating gold in the 1976 Winter Olympics in Innsbruck, Austria. At nineteen years old, Hamill was thrust into the spotlight and mobbed for autographs. She was a star, but she didn't feel like one. "When you have that goal and you have that dream and it actually happens, you think that it would be a switch," she told CBS News correspondent Thalia Assuras. "And that all of a sudden you'd feel, you know, like an Olympic champion. And I didn't feel any different." 













 Hormonal fluctuations in both women and men account for their aberrations in their thinking, behavior, moods, and their sexuality, expressed in the symptoms of
Hormonal fluctuations in both women and men account for their aberrations in their thinking, behavior, moods, and their sexuality, expressed in the symptoms of 


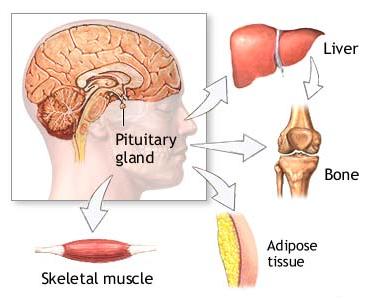 The decline of our fundamental hormones is directly associated with certain aging signs like shrinkling of the skin, graying of the hair, decreased energy and sexual function, increased body fat, heart disease, weak and brittle bones, and much more. The good news is that
The decline of our fundamental hormones is directly associated with certain aging signs like shrinkling of the skin, graying of the hair, decreased energy and sexual function, increased body fat, heart disease, weak and brittle bones, and much more. The good news is that 
 7-keto DHEA
7-keto DHEA
 Thousands of scientific articles have been published about this powerful hormone’s
Thousands of scientific articles have been published about this powerful hormone’s 
 A small number of men have lost eyesight in one eye some time after taking Viagra, Cialis, or Levitra. This type of vision loss is called non-arteritic anterior ischemic optic neuropathy (NAION). NAION causes a sudden loss of eyesight because blood flow is blocked to the optic nerve.
A small number of men have lost eyesight in one eye some time after taking Viagra, Cialis, or Levitra. This type of vision loss is called non-arteritic anterior ischemic optic neuropathy (NAION). NAION causes a sudden loss of eyesight because blood flow is blocked to the optic nerve. 
